JADA Uses Vacuum to Induce Physiologic Contraction of the Uterus1
The majority of postpartum hemorrhage cases are caused by uterine atony.2,*
See JADA in Action
Fast, Physiologic Control of Abnormal Postpartum Uterine Bleeding2
The JADA System is intended to provide control and treatment of abnormal postpartum uterine bleeding or hemorrhage when conservative management is warranted.
The JADA System with low-level vacuum connected
The uterus is composed of a web-like network of muscle fibers in its middle layer, called the myometrium. When the placenta separates from the uterine wall after childbirth, that portion of the myometrium is left with open blood vessels, resulting in bleeding. Typically, the uterus contracts and compression of those open vessels stops bleeding. In some instances, the uterine muscle fibers do not contract, causing uncontrolled bleeding, referred to as abnormal postpartum uterine bleeding or postpartum hemorrhage.2
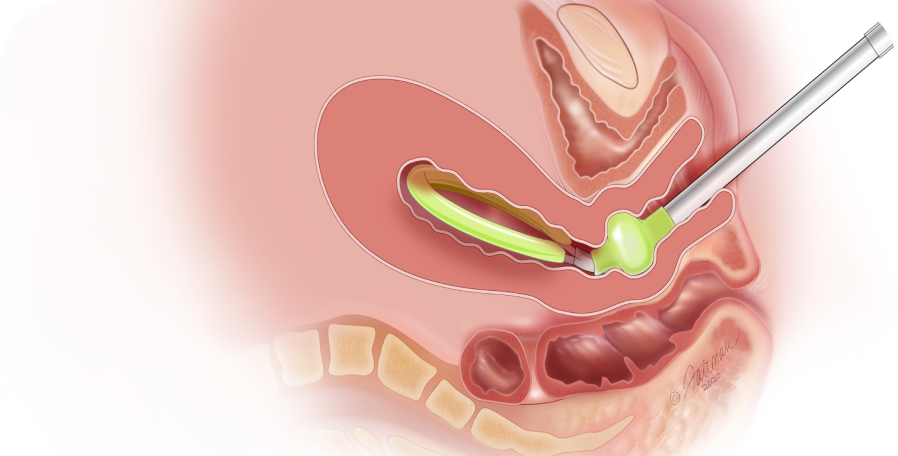
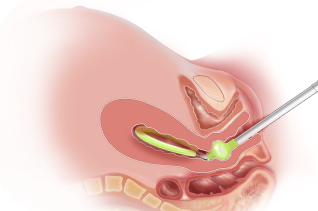
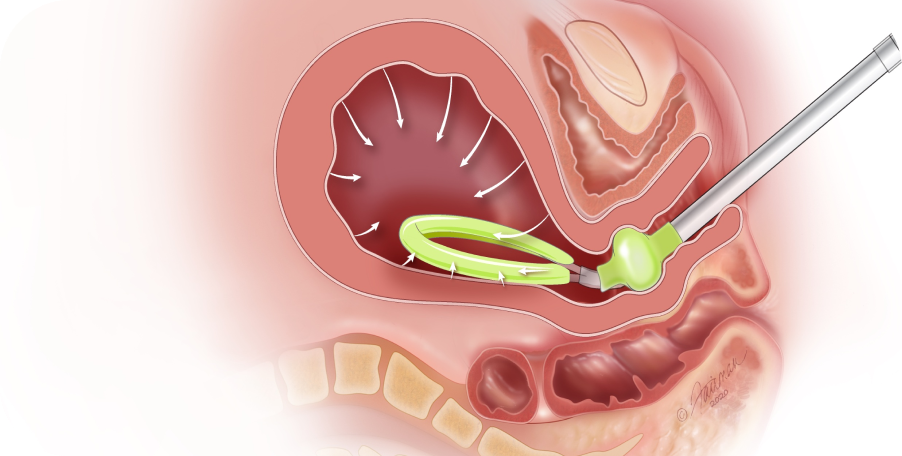
Uterine contraction with the JADA System
When connected to a low-level vacuum source (80 mm Hg +/- 10 mm Hg; not to exceed 90 mm Hg), JADA establishes a vacuum within the uterus, causing the uterus to contract and leading to control of the bleeding. In a clinical study (n=107), contraction of the uterus was observed in a median of 1 minute with control of bleeding observed in a median of 3 minutes.2
Innovation That Works


JADA is made of silicone and a survey found that it is easy to use (98%, n=105/107).2


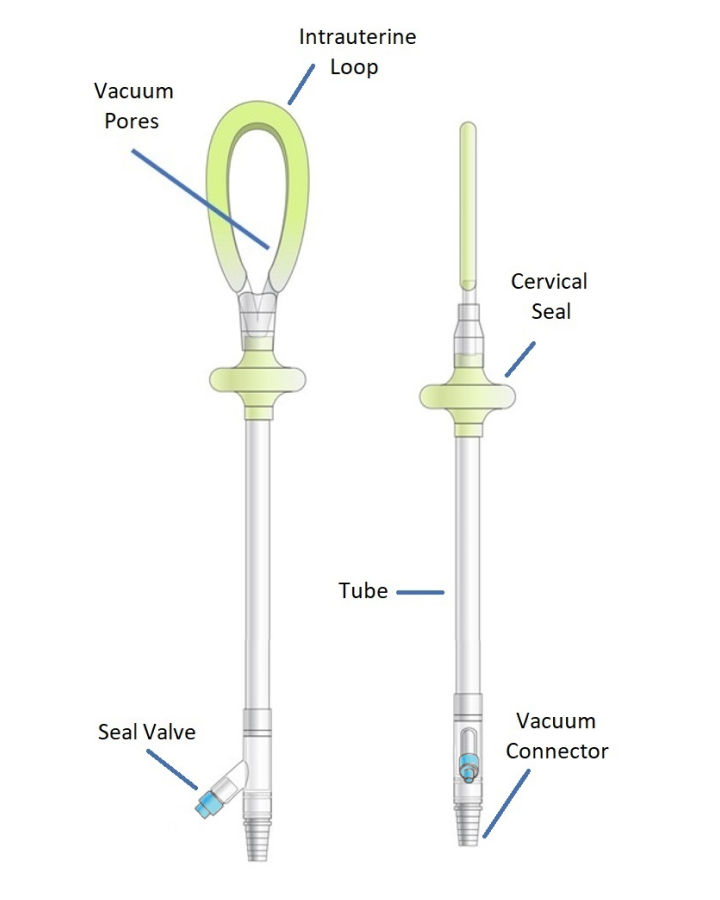
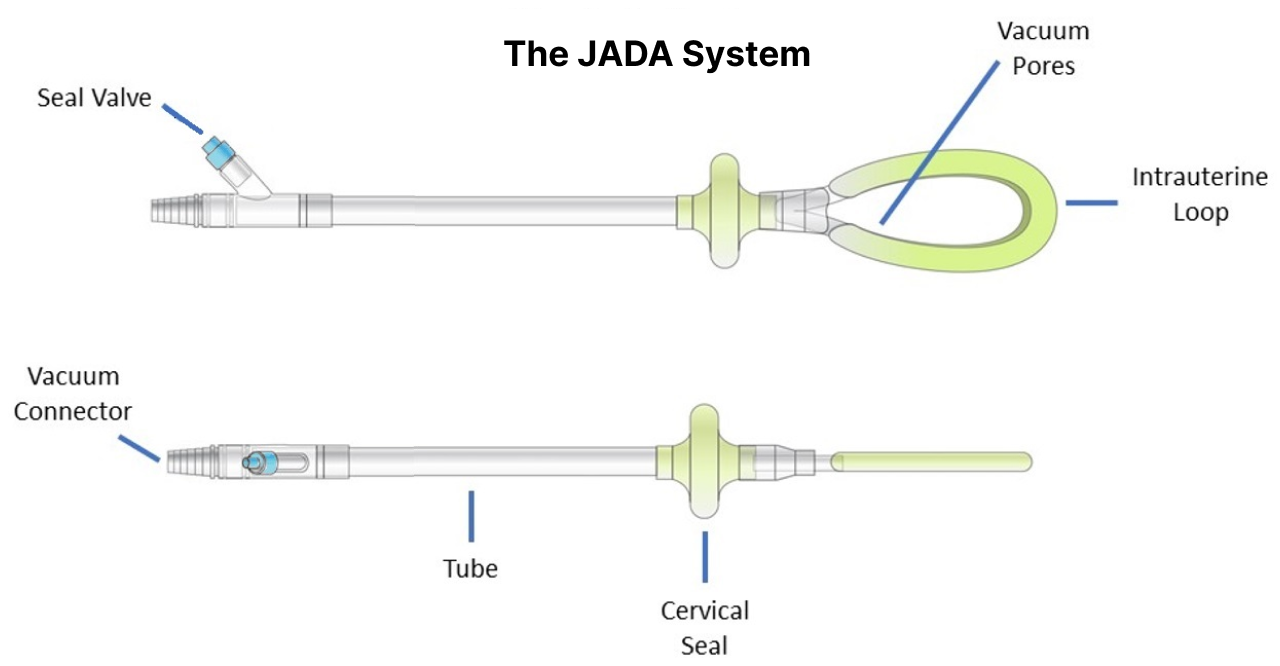
An Intrauterine Loop has interior Vacuum Pores inside a protective Shield to evacuate blood.


An expandable Cervical Seal is filled with sterile fluid to create a seal that holds a vacuum within the uterus.
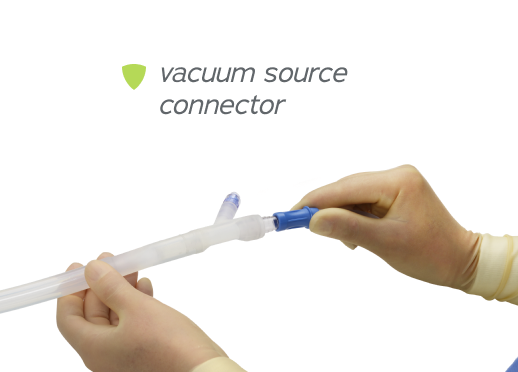

A connector at the end of the tube is attached to a regulated vacuum source.
Before using JADA, please read the contraindications, warnings, precautions, and other important information in the accompanying Instructions for Use.
Contraindications and Warnings
Contraindications
- Ongoing intrauterine pregnancy
- Untreated uterine rupture
- Unresolved uterine inversion
- Current cervical cancer
- Known uterine anomaly
- Current purulent infection of vagina, cervix, or uterus
- For C-sections: Cervix < 3 cm dilated before use of JADA
Warnings
- Avoid excessive force when inserting the JADA into the uterus or trauma to uterine wall may occur, including perforation.
- The safety and effectiveness of the JADA System in delivery at a gestational age < 34 weeks or, if multiples, uterus judged < 34 weeks size, have not been established. With smaller uterine size, there is potential for increased risk of perforation and expulsion.
- Signs of patient deterioration or failure to improve indicate the need for reassessment and possibly more aggressive treatment and management of postpartum hemorrhage (PPH)/abnormal postpartum uterine bleeding.
- JADA is not a substitute for surgical management and fluid resuscitation of life-threatening PPH/abnormal postpartum uterine bleeding.
- Remove air from Cervical Seal prior to device use to minimize risk of air embolism if Cervical Seal bursts.
- Always fill the Cervical Seal with sterile fluid. Never inflate with air, carbon dioxide, or any other gas to minimize risk of air embolism if Cervical Seal bursts.
Get in Touch
If you are a healthcare professional interested in bringing JADA to your facility, click below to be contacted by the representative in your area.